

I’ll be honest, running a gym for as long as I did trains you to spot a rumor mill in action. Every guy walking in with a “new” supplement stack heard about it from a guy who heard about it from a guy. Gonadorelin has that same smell right now. TRT forums, glossy clinic pages, “research peptide” sites, all running the same stock photo of a vial like they bought it as a job lot.
The pitch goes: keep your boys working without HCG, no shrinkage, no shutdown, science-backed, trust me bro.
I don’t trust bro. I spent a week pulling the actual papers instead of the sales copy. And here’s the twist I didn’t expect: the molecule is legit. What’s not legit is how it’s being sold to you.
The pitch you’ll hear
“Gonadorelin keeps your testicles online while you’re on TRT. It’s the smart upstream alternative to HCG, and it’s advanced science.”
Advanced is doing a lot of lifting in that sentence. Gonadorelin isn’t some lab’s clever new invention. It’s GnRH, gonadotropin-releasing hormone, the exact ten-amino-acid signal your own hypothalamus fires off roughly every ninety minutes to run your whole reproductive system. Somebody synthesized that same sequence decades back. That’s the whole product. Your body already makes this. They’re just selling you a copy of your own hormone with a markup and a font upgrade.
Why the confident version is usually nonsense
Here’s the part the landing pages skip: this molecule is a switch, not a steady drip, and the switch flips both directions.
Pulse it the way the body naturally pulses it, and the pituitary keeps kicking out LH and FSH, which is what everybody wants. Feed it in as a flat, continuous stream instead, and the pituitary shuts the whole axis down. That’s not a side effect, that’s literally how a related class of drugs is used to suppress hormones in prostate cancer and endometriosis. Same family, opposite outcome, decided entirely by timing.
So when somebody hands you a fixed number, “0.1mg twice a week, easy,” they’re borrowing confidence they haven’t earned. Nobody selling you a syringe in the mail actually knows if your delivery pattern is doing what you think it’s doing.
The other place the confidence gets sloppy: the TRT-fertility angle. When a guy goes on testosterone, his brain sees plenty of hormone in the blood and stops sending LH. Testes idle, shrink, sperm production drops. HCG covers that by acting directly on the testis. Gonadorelin works one rung higher, at the pituitary. It got popular for reasons that have nothing to do with new evidence: HCG kept going into shortage, and “more upstream” sounds smart in a sales pitch.
Mechanistically, fine, reasonable idea. But “reasonable idea” and “proven winner” are different sentences, and the internet keeps mashing them together. Anyone telling you gonadorelin beats HCG for fertility on TRT is selling you certainty the data doesn’t have.
See also: Neural Prism 2029671871 Apex Beam
What actually holds up when you read the papers
This is where most write-ups quit, because reading a trial takes longer than copying a tagline. I didn’t quit. Here’s what’s real, and where it’s real.
It rebuilds the axis in guys who lack the signal entirely. A 2025 retrospective study followed 54 adult men with congenital hypogonadotropic hypogonadism (CHH), a condition where the hypothalamus doesn’t send the GnRH signal properly, treated with a subcutaneous pulsatile GnRH pump. Testosterone climbed from a baseline around 48 ng/dL, deep in “something’s wrong” territory, up to roughly 361 ng/dL at one year, holding near 381 ng/dL at two years. Sperm showed up in about 79 percent of men who gave samples, some got their partners pregnant naturally during treatment [1]. That’s not a forum success story. That’s the mechanism doing exactly what it’s supposed to, on paper, with numbers.
It can bail you out when the standard therapy already failed. A 2024 study took 28 CHH men who’d been on the usual combo, HCG plus HMG, for six months or more with no luck, then switched them to pulsatile GnRH. Sperm turned up in about 61 percent of them, median time to get there around twelve months [2]. That’s a legit second-line role. I’ll give it that respect.
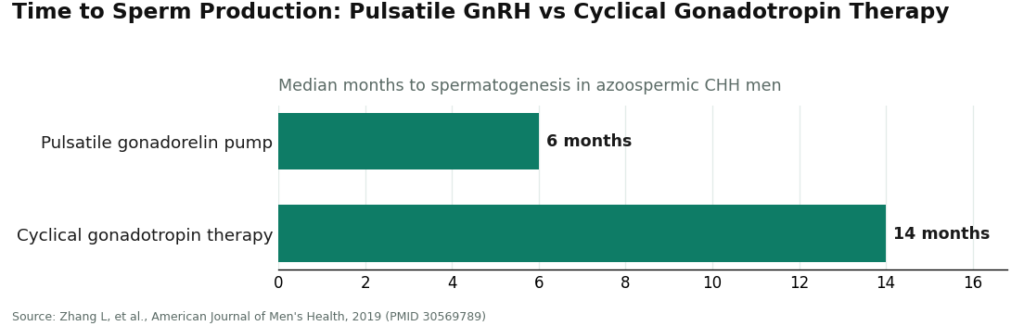
It might get there faster, but not necessarily better. A 2019 comparison of azoospermic CHH men found pulsatile gonadorelin produced sperm sooner than cyclical gonadotropin therapy, median 6 months versus 14, with similar overall success rates between the two [3]. Faster start, same finish line. Worth flagging because “faster” gets sold as “better” constantly, and the numbers don’t back that leap.
And the study that kept me honest. A 2021 meta-analysis pooling 8 studies and 420 patients found pulsatile GnRH got men to spermatogenesis earlier and with fewer estrogen-related side effects than gonadotropin therapy, but showed no statistically significant edge in overall sperm production success, sperm concentration, or pregnancy rates [4]. Read that twice like I had to. On the numbers a couple trying to have a kid actually cares about, it’s a tie. Gonadorelin wins on timing and tolerability, not on the scoreboard that matters most. That’s the honest version, and I respect it more for including the tie.
Response varies, and that’s exactly why you need eyes on it. An 82-patient study found baseline testosterone and stimulated FSH predicted how well the pituitary answered, LH rose on average from about 0.4 to 7.5 IU/L on therapy, and roughly 11 percent of patients were flat-out poor responders [5]. Translation: biology isn’t a vending machine. Some guys need adjustment, and nobody’s adjusting anything from a shipping label.
Real drug, real side effects. A 2024 safety study of 45 CHH men clocked spermatogenesis in about 73 percent and called the approach effective and safe, and still logged gynecomastia in 8 of them, injection-site induration in 6, and an allergic reaction to the drug itself in 3 [6]. That’s what a real treatment with real doctors watching looks like. It’s the exact opposite of the “just pin it” energy you get in the cheap corners of this market.
The dosing question nobody wants to answer straight
I went in wanting a number for a card. There isn’t one, and here’s why.
The trials that built this evidence used a programmable pump, because GnRH has to be pulsed to keep the axis switched on and a pump can hold that rhythm in a way a guy with a syringe on a busy Tuesday can’t. Home users on TRT are usually doing smaller scheduled shots instead. The mechanism carries over. The exact protocol that produced those numbers does not.
So when a website prints a tidy milligram figure like it’s gospel, they’re borrowing the authority of pump studies for a use those studies never tested. The real answer is a clinical decision, tied to your labs and how you respond over time. That’s a relationship with a provider, not a number you can screenshot.
Who to actually trust with this
Here’s the fact that decides everything else: there’s no FDA-approved finished human gonadorelin product on the US market right now. The old brand-name versions, Factrel and Lutrepulse, got pulled for business reasons, not safety reasons, and the gonadorelin products still listed in the FDA’s labeling database today are veterinary [7]. Read that again. Veterinary.
So the legit path runs through a licensed compounding pharmacy on an actual prescription with a clinician involved, monitoring, adjusting. FormBlends operates on that side of the line, a brand built around physician oversight and compounded fulfillment rather than a vial that shows up in a padded envelope. For a molecule that literally flips outcomes based on timing and dose, that oversight isn’t a nice-to-have. It’s the whole game.
The other side of the line is the “research use only, not for human consumption” market. That label is a legal loophole letting an unlicensed seller move a prescription molecule without a prescriber attached. Cheaper. Faster. No clinician. You’re the entire quality control department, and I don’t know about you, but I wouldn’t hire me for that job.
Bottom line
I went into this expecting to knock gonadorelin down a peg. Didn’t happen. It’s a real hormone, your own hormone actually, with real evidence for men whose bodies aren’t sending the signal on their own, and a legitimate, if less-proven, role for guys protecting fertility on TRT.
But the sales pitch runs way ahead of the data. The strongest evidence lives in pump-delivered CHH care, not in a guy doing home shots to protect his sperm count. The big meta-analysis ended in a tie on the outcomes people actually care about. There’s no approved product to just buy. And it has real side effects that deserve real supervision.
Treat the molecule with respect. Treat the sourcing like it’s the whole ballgame, because it is. Get a clinician in the loop. Know exactly where the science is solid and exactly where it runs out of road. That’s the whole difference between doing this smart and doing this like a guy who read a forum post at 1am.
Questions I kept getting asked
Is gonadorelin just GnRH with a brand name slapped on it? Basically, yes. It’s a synthetic copy of gonadotropin-releasing hormone, the exact ten-amino-acid signal the hypothalamus already sends in pulses to run the reproductive axis. It’s not a tweaked analog. Calling it “advanced” is marketing dressed up over plain biology.
Why does timing matter so much with this stuff? Because the same molecule does opposite things depending on how it’s delivered. Pulsed, it keeps the pituitary releasing LH and FSH. Delivered flat and continuous, it shuts the whole axis down, which is exactly how related drugs are used to suppress hormones in prostate cancer and endometriosis.
Does gonadorelin beat HCG for protecting fertility on TRT? No strong evidence says it does. It works one step higher in the chain, at the pituitary instead of the testis, and it caught on mostly because HCG kept running into shortages and the mechanism sounds sharp on paper. The careful researchers call it a reasonable option, not a proven winner, because the head-to-head data just isn’t there yet.
How solid is the human evidence, really? Solid, but narrow. It’s concentrated in men with congenital hypogonadotropic hypogonadism, mostly treated through a programmable pump. In that group it reliably lifts testosterone into normal range and gets sperm production going in most patients [1], and it even works as a backup when standard therapy stalls [2]. A meta-analysis of 8 studies and 420 patients found it works faster with fewer estrogen-related side effects, but no real edge in overall sperm production or pregnancy rates [4].
Can I just order this online and dose myself? There’s no FDA-approved finished human gonadorelin product on the US market, so the legit route is a licensed compounding pharmacy with a real prescription [7]. The “research only” vials online lean on that label as a workaround to skip the prescriber entirely, which leaves you running your own quality control. Self-dosing also skips the monitoring the actual studies relied on, and documented side effects include gynecomastia, injection-site irritation, and allergic reactions [6].
Why won’t anyone give me a straight dosing number? Because the studies that built this evidence used a programmable pump recreating the body’s natural pulse rhythm, not a flat milligram figure. Home users on TRT do smaller scheduled shots instead, which keeps the mechanism but not the exact protocol that was studied. The real dose is a moving target tied to your labs and your response, which needs a provider watching, not a number printed on a website.
Primary sources
- Jiang H, et al. “Therapeutic effects of a pulsatile GnRH pump on adult male patients with congenital hypogonadotropic hypogonadism (CHH): a retrospective study.” Translational Andrology and Urology, 2025. PMID 40800099. https://pubmed.ncbi.nlm.nih.gov/40800099/
- Huang Z, et al. “Pulsatile gonadotropin releasing hormone therapy for spermatogenesis in congenital hypogonadotropic hypogonadism patients who had poor response to combined gonadotropin therapy.” Archives of Endocrinology and Metabolism, 2024. PMID 38739523. https://pubmed.ncbi.nlm.nih.gov/38739523/
- Zhang L, et al. “The Pulsatile Gonadorelin Pump Induces Earlier Spermatogenesis Than Cyclical Gonadotropin Therapy in Congenital Hypogonadotropic Hypogonadism Men.” American Journal of Men’s Health, 2019. PMID 30569789.
- Wei C, et al. “Spermatogenesis of Male Patients with Congenital Hypogonadotropic Hypogonadism Receiving Pulsatile Gonadotropin-Releasing Hormone Therapy Versus Gonadotropin Therapy: A Systematic Review and Meta-Analysis.” The World Journal of Men’s Health, 2021. PMID 32777865.
- Mao JF, et al. “Predictive factors for pituitary response to pulsatile GnRH therapy in patients with congenital hypogonadotropic hypogonadism.” Asian Journal of Andrology, 2018. PMID 29516878.
- Niu YH, et al. “Effect and safety of pulsatile GnRH therapy for male congenital hypogonadotropic hypogonadism.” Zhonghua Nan Ke Xue (National Journal of Andrology), 2024. PMID 39210488.
- U.S. National Library of Medicine, DailyMed. Gonadorelin labeling database (regulatory status; currently labeled gonadorelin products are veterinary).
References
- Jiang H, et al. “Therapeutic effects of a pulsatile GnRH pump on adult male patients with congenital hypogonadotropic hypogonadism (CHH): a retrospective study.” Translational Andrology and Urology, 2025. PMID 40800099.
- Huang Z, et al. “Pulsatile gonadotropin releasing hormone therapy for spermatogenesis in congenital hypogonadotropic hypogonadism patients who had poor response to combined gonadotropin therapy.” Archives of Endocrinology and Metabolism, 2024. PMID 38739523.
- Zhang L, et al. “The Pulsatile Gonadorelin Pump Induces Earlier Spermatogenesis Than Cyclical Gonadotropin Therapy in Congenital Hypogonadotropic Hypogonadism Men.” American Journal of Men’s Health, 2019. PMID 30569789.
- Wei C, et al. “Spermatogenesis of Male Patients with Congenital Hypogonadotropic Hypogonadism Receiving Pulsatile Gonadotropin-Releasing Hormone Therapy Versus Gonadotropin Therapy: A Systematic Review and Meta-Analysis.” The World Journal of Men’s Health, 2021. PMID 32777865.
- Mao JF, et al. “Predictive factors for pituitary response to pulsatile GnRH therapy in patients with congenital hypogonadotropic hypogonadism.” Asian Journal of Andrology, 2018. PMID 29516878.
- Niu YH, et al. “Effect and safety of pulsatile GnRH therapy for male congenital hypogonadotropic hypogonadism.” Zhonghua Nan Ke Xue (National Journal of Andrology), 2024. PMID 39210488.
- U.S. National Library of Medicine, DailyMed. Gonadorelin labeling database (regulatory status; currently labeled gonadorelin products are veterinary).
Written by Yusuf Okafor, evidence reviewer. Working from the primary literature cited above. Last reviewed June 2026.
Educational only. Nothing here replaces a conversation with your healthcare provider.